
Sciatica: Beyond the Pain, Finding the Cause
40% of people will experience sciatica at some point in their lives. Yet despite its prevalence, sciatica remains one of the most misunderstood conditions—often conflated with general back pain and frequently mismanaged with prolonged rest. The good news? Research shows that 85-90% of sciatica cases resolve with conservative care, without the need for surgery. At PhysioMotion, we take a targeted, evidence-based approach to identify the root cause of your symptoms and guide you back to pain-free movement.
Understanding Sciatica
What is Sciatica?
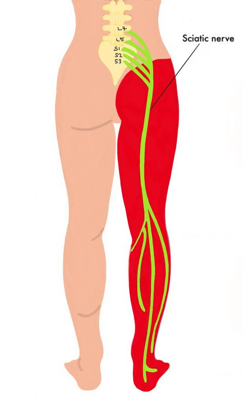
Sciatica is not a diagnosis in itself - it is a symptom of nerve irritation or compression specifically of the sciatic nerve itself. It is the largest nerve in the body, running from your lower back, through the buttock, and down the back of each leg. The hallmark of true sciatica is pain that travels below the knee.
Common Causes of Sciatica
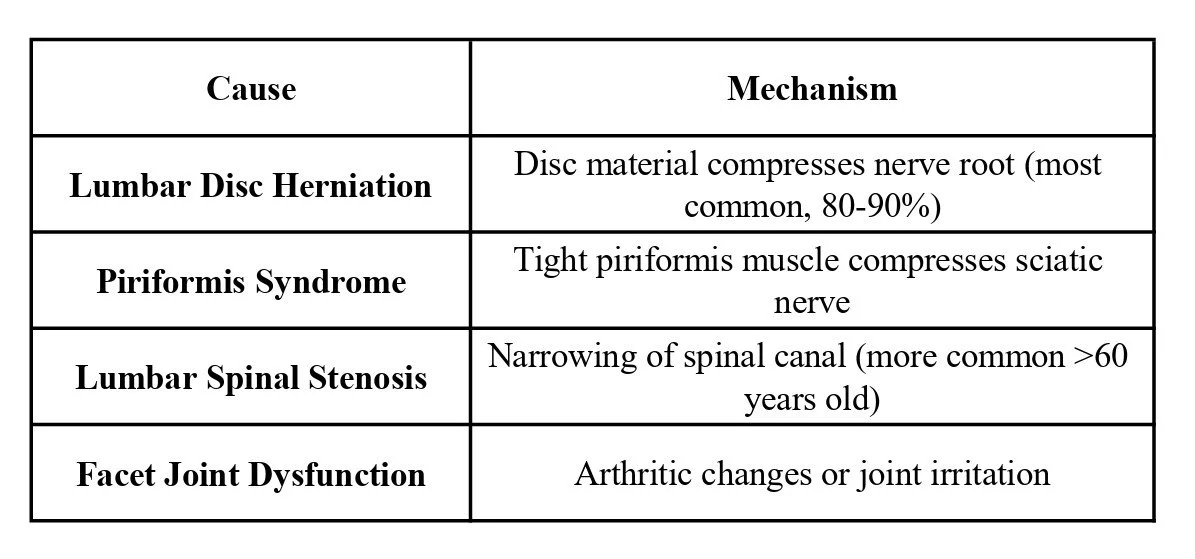
Source: Koes et al., 2007, The Lancet
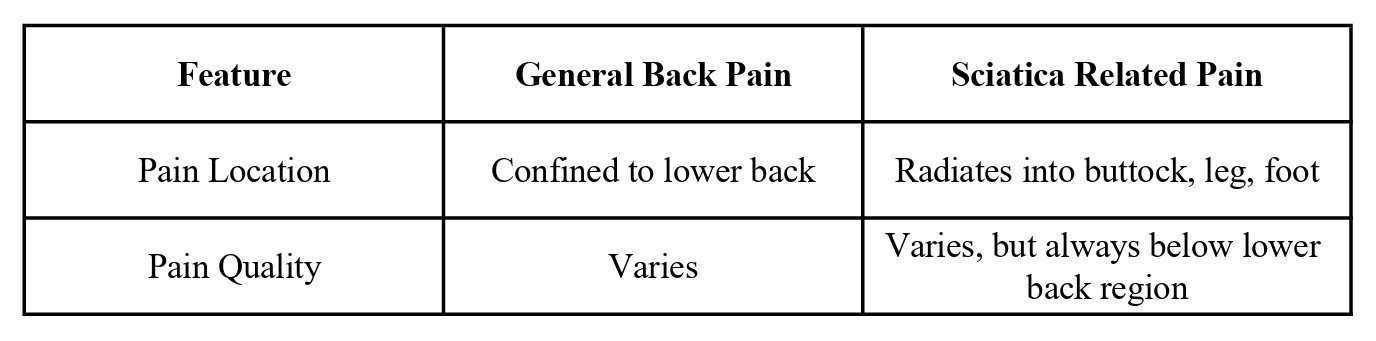
Differentiating Sciatica from General Back Pain
Red Flags & When to Refer
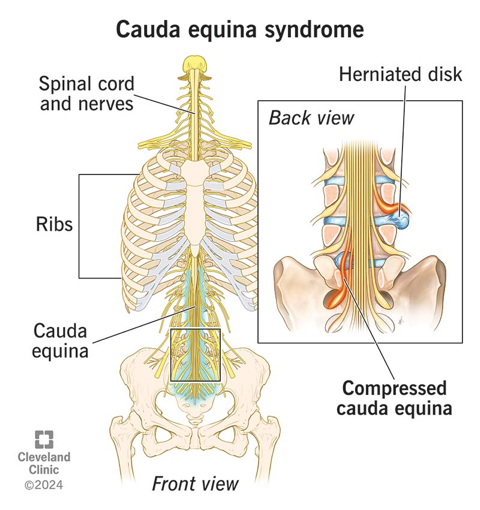
Cauda Equina Syndrome – Urgent Surgical Emergency
Cauda Equina Syndrome (CES) is a medical emergency requiring immediate surgical intervention.
Red Flag Signs-Seek Emergency Care:
Saddle anesthesia: Numbness in groin, buttocks, inner thighs
Bladder dysfunction: Urinary retention (unable to urinate) or sudden severeincontinence (loss of control of the bladder)
Bowel dysfunction: Sudden Fecal incontinence (loss of bowel control)
Bilateral leg symptoms: Progressive prolonged and severe weakness in both legs
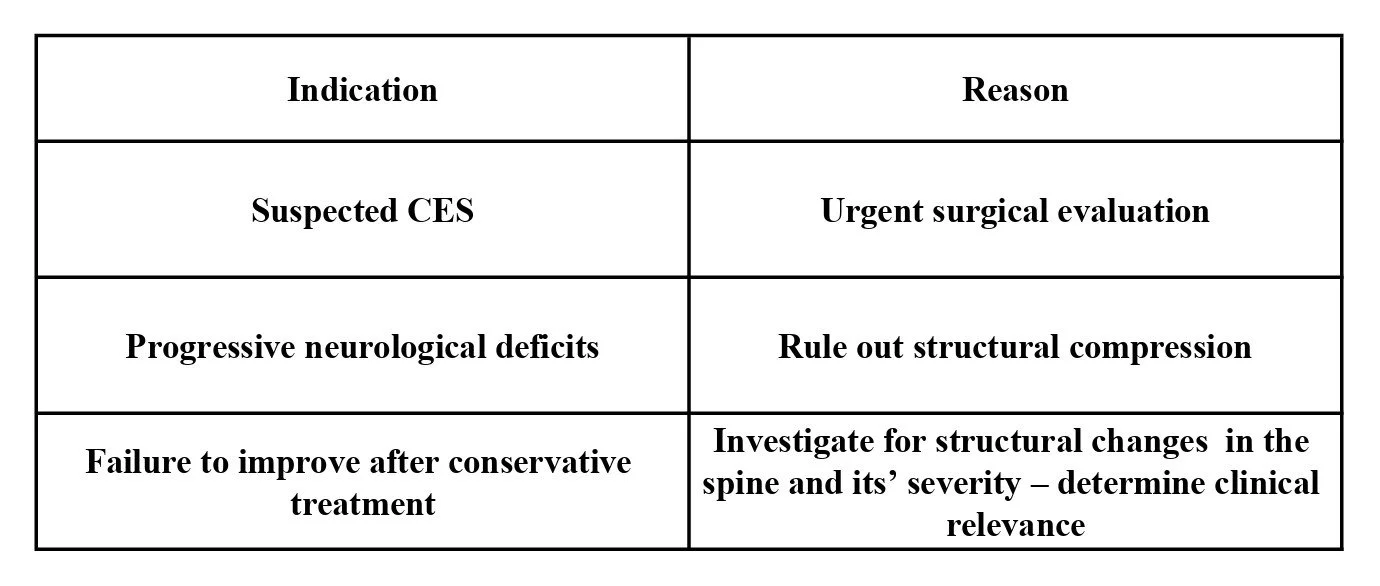
When Imaging is Necessary
Q&A: Common Sciatica Questions Answered
Q: Does sciatica always require surgery?
A: No. 85-90% of patients improve within 6-12 weeks with conservative care (Lewis et al., 2021). Surgery is reserved for CES, progressive neurological deficits, or failure to respond to conservative treatment
Q: Why does my leg hurt more than my back?
A: This is a classic sign of nerve root irritation. When a nerve is compressed, symptoms are often felt distally (further down the nerve) rather than at the site of compression—common in disc herniations. Very important to find the underlying reason as to what regions of the body are causing excessive load on the spine, disc and nerve root to cause this irritation. Treat these causes and pain will most likely resolve because this will 'offload' the nerve irritation and compression.
Q: Can sitting make sciatica worse?
A: Yes. Sitting increases intradiscal pressure by 30-40% compared to standing (Wilke et al., 1999). Prolonged sitting also compresses the piriformis muscle and increases tension on the sciatic nerve. In particular, poor posture when sitting.
Q: How long does recovery typically take?
A: Most patients see significant improvement in 2-4 weeks with appropriate care. 85-90% recover within 6-12 weeks with conservative management.
Our Physiotherapy Approach to Sciatic pain

Phase 1: Comprehensive Assessment
We identify the root cause through movement analysis, nerve tension testing (straight leg raise, slump test), neurological examination, postural screening and lifestyle evaluation.
Phase 2: Manual Therapy
Mobilization and manual therapy including soft tissue release techniques combined with dry needling / acupuncture to the region of the body that is causing the excessive loading on the spine, discs and sciatic nerve
Phase 3: Nerve Mobilization
A 2022 systematic review found that nerve mobilization significantly reduces pain and disability in patients with radicular pain. Gentle gliding techniques allow the nerve to move freely, reducing adhesion and inflammation.
Phase 4: Core & Stability Retraining
Deep core activation (transverse abdominis, multifidus) or 'core muscle' training for any contributory regions
Integrating whole body global strength with dynamic stability of core areas
Progressive loading as pain subsides
Phase 5: Ergonomic & Lifestyle Advice
Sitting: Optimal ergonomics with frequent movement breaks every hour
Sleeping: Side-lying with pillow between knees; back-lying with pillow under knees when in acute pain
Activity: Gentle walking; avoid prolonged sitting and heavylifting in acute phases
Key Takeaways:
Sciatica is a symptom, not a diagnosis. Identifying the underlying cause is essential.
85-90% of cases resolve with conservative care. Surgery is reserved for specific indications.
Movement is medicine, not rest. Graded, guided movement is superior for healing.
Early physiotherapy reduces chronicity and recurrence. Targeted care in the first weeks significantly improves outcomes.
Consistent & regular exercise. This maintains joint mobility and muscle strength to support your body